Issue 16: Boys' Victimization & Adult IPV Perpetration
 Printable PDF Version
Printable PDF Version
View Plaintext PDF
Research indicates that approximately 1 in 6 maltreated boys go on to perpetrate violence.1 Yet, men’s childhood experiences with abuse, neglect, and exposure to intimate partner violence (IPV) are often under-recognized and subsequently remain untreated.2
Why is the victimization of boys an important issue to understand in the prevention of gender-based violence?
Men comprise over 80% of perpetrators of violence against women in Canada, and one key risk factor for the perpetration of IPV is the experience of neglect, abuse, or exposure to IPV in childhood (referred to from this point forward as child maltreatment).3
Of course, not all boys who experience violence as children become perpetrators of IPV, and not all men will use or condone gender-based violence.
Nevertheless, prevention efforts cannot overlook the increasing evidence of an association between the two.
There are a wide range of factors involved in IPV perpetration. This newsletter draws attention to the ways in which IPV prevention can be enhanced through identifying men at risk of becoming perpetrators at earlier points in their lives. It is possible that the impacts of boys’ experiences of violence can be minimized through age-specific intervention programs. In turn, this may reduce the proportion of these boys who go on to perpetrate violence against their partners as they grow older.
Taking a Life Course Perspective
- Human development is a lifelong process.
- Children’s lives are intricately linked to those of their parents or caregivers.
- Early life experiences influence subsequent life outcomes.
- Context matters (e.g. culture, access to resources).
- “Turning points” are possible.
Forms of Child Maltreatment and Definitions4
| Physical abuse | Any act of physical aggression directed toward a child (e.g. shaking, pushing, hitting with object, biting, choking). |
| Sexual abuse | Sexual molestation or exploitation of a child by an adult or older child within or outside the family (e.g. penetration, fondling, pornography). |
| Emotional/psychological abuse | Terrorizing or threat of violence (e.g. threats against child’s cherished objects), verbal abuse or belittling (e.g. name-calling), isolation or confinement (e.g. purposely cutting child off from other children), inadequate nurturing or affection (e.g. lack of parental interaction), exploiting or corrupting behaviour (e.g. encouraging involvement in criminal behaviour). |
| Neglect | Failure to provide for child’s basic needs, adequate protection, and adequate supervision (e.g. inadequate nutrition, failure to provide medical treatment). |
| Exposure to intimate partner violence |
Child is present during physical or verbal violence between intimate partners and can see and/or hear the violence (direct); child not present during violence but suffers consequences, hears about it, or experiences changes in his/her life as a result (indirect); child is exposed to emotional violence between intimate partners. |
IPV Perpetration & Child Maltreatment: Shared Risk Factors
IPV and child maltreatment are inter-related forms of violence. In fact, over 33% of children exposed to IPV in the past year also experienced maltreatment, compared to just 9% of children with no IPV exposure.5 Not surprisingly, there are many common risk factors between IPV perpetration and child maltreatment perpetration.
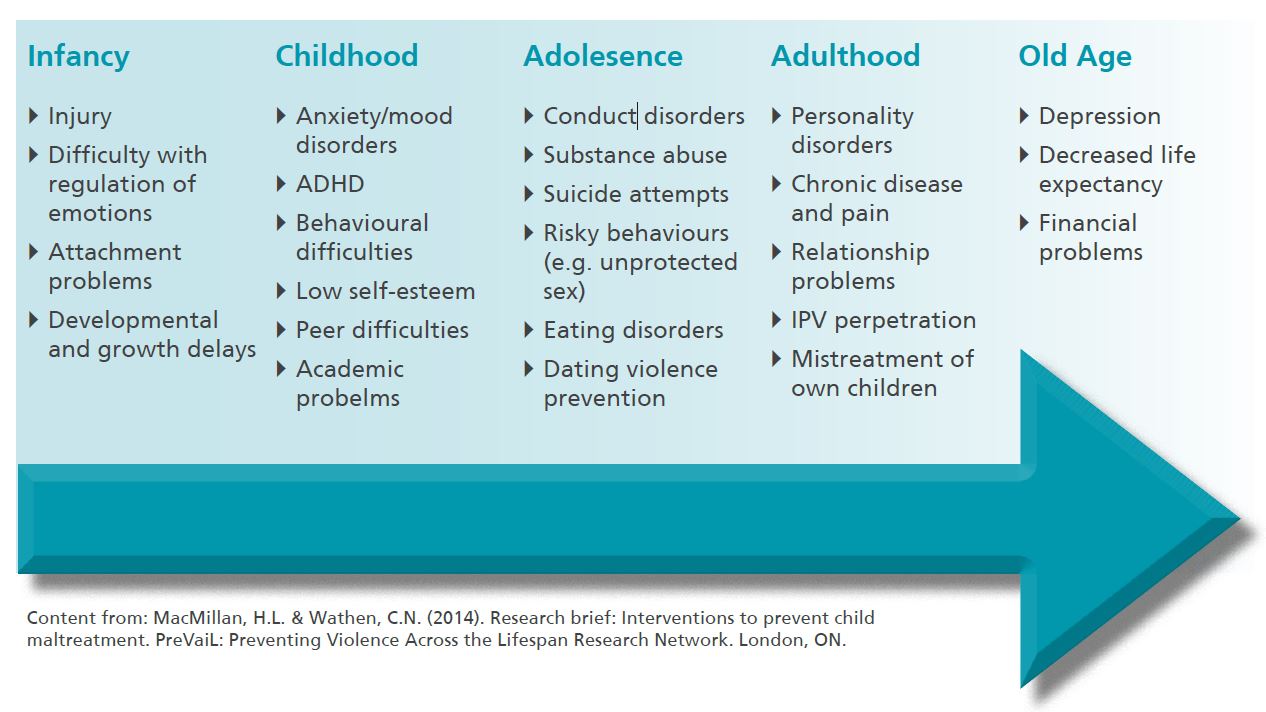
Associated Consequences of Family Violence Across the Life Course
Both child maltreatment and IPV are associated with many adverse effects on health and well-being across the life course, situating these forms of violence as public health issues requiring concentrated prevention efforts. Examples of the impacts of violence are pictured below.
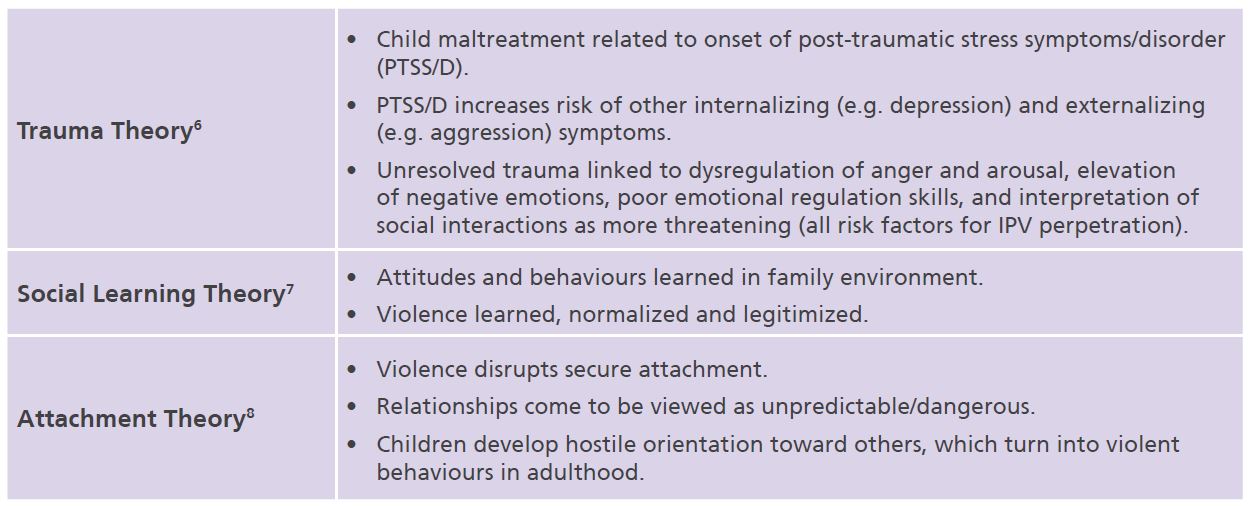
Theoretical Frameworks
There are many proposed explanations for the link between boys’ experiences of violence and future perpetration of IPV. Three of these explanations are listed below.
What does the Evidence Tell Us?
The relationship between experiencing maltreatment in childhood and perpetrating IPV in adulthood is generally supported by cross-sectional and longitudinal evidence from a large number of rigorous studies spanning across many populations.9 For a review, see our full report here.
Longitudinal research supports cross-sectional findings and indicates boys who have experienced maltreatment have a higher risk for perpetrating violence against women as they grow older than boys with no such experiences. Findings also reveal that young adulthood may be a key timeframe for the emerging effects of child maltreatment.
Many studies link child maltreatment to dating or intimate partner violence in adolescence and young adulthood or find that child maltreatment predicts youth violence, which in turn, predicts IPV perpetration.
Research Highlights
- One large national survey found that men’s risk of perpetrating IPV increased by 58 to 64%, depending on the type of maltreatment they experienced as boys – sexual abuse, IPV exposure, or physical abuse (Roberts et al., 2011).
- Results from one prospective study revealed exposure to IPV prior to age 5 directly predicts IPV perpetration at age 23 (Narayan et al., 2013).
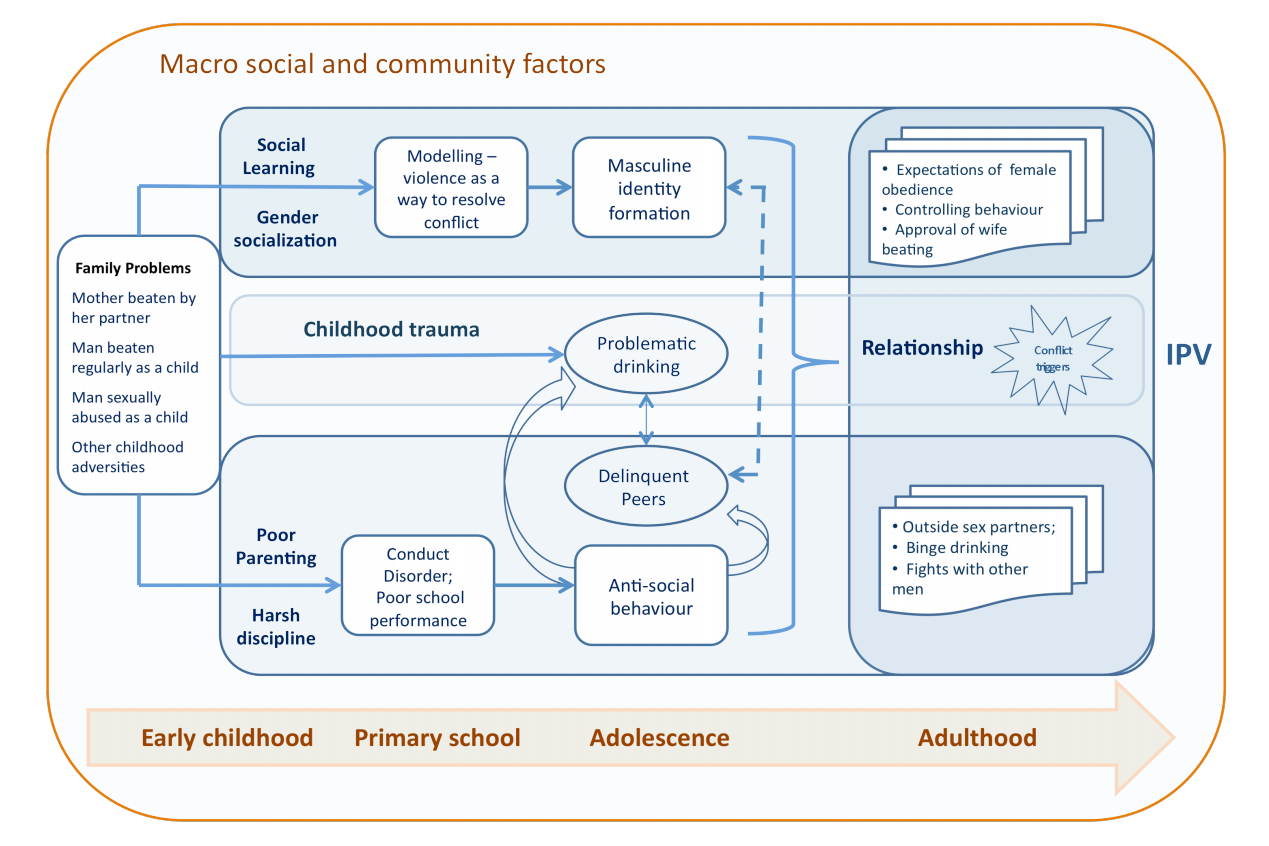
Pathways to Perpetration: Situating boys' and men's experiences of violence
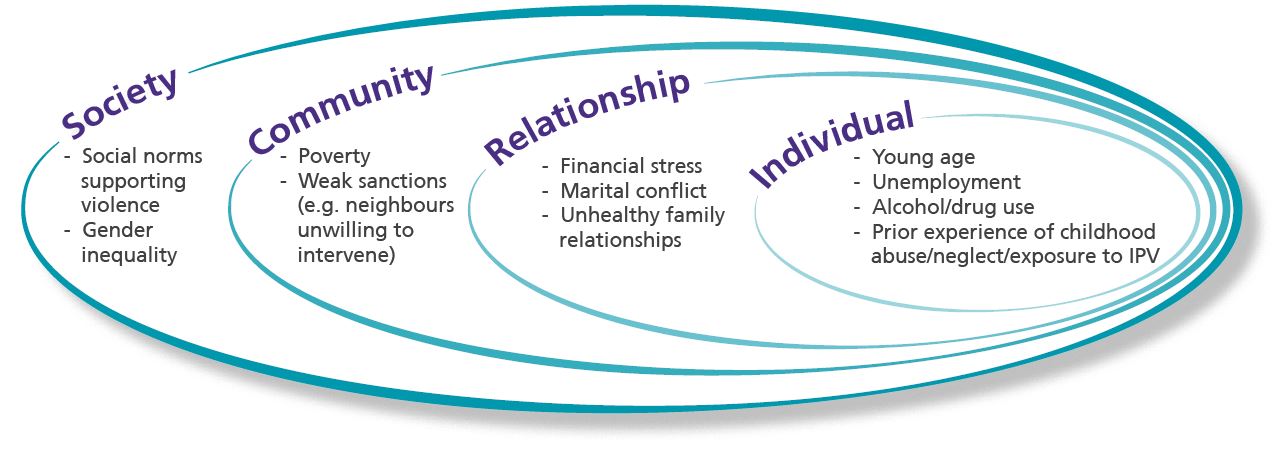
Pathways to IPV perpetration are complex and require a multifaceted approach to prevention. When examining prevention by life stage, it is important to consider co-existing and contextual risk factors:
Prevention across the Life Course
We reviewed evidence-based prevention strategies with results from randomized control trials10, and to a lesser extent, strategies with emerging evidence that are considered promising.
Findings include:
- Interventions at each life stage can impact risk factors associated with men’s perpetration of IPV (e.g. insecure attachment, child behaviour problems, trauma symptoms) in addition to reducing child abuse, neglect, and IPV exposure.
- 6 evidence-based programs have applications across life stages (e.g. Traumafocused Cognitive Behavioural Therapy).
- Most of the reviewed programs involve secondary or tertiary prevention efforts.
- There is a need for further evaluation of primary prevention programs in adolescence and adulthood.
Levels of Prevention
Primary prevention: aims to intervene before the occurrence of IPV by preventing the development of associated risk factors, such as child maltreatment.
Secondary prevention: targeted to individuals at high risk of experiencing or perpetrating child maltreatment or IPV, with the goal of preventing its occurrence or progression.
Tertiary prevention: occurs after child maltreatment or IPV has been identified, with interventions designed to minimize its impact for survivors and decrease the risk of recurring abuse.
Evidence-based Prevention Programs
Click on the program names for more information!
| Infancy/Pre-School | School-Age | Adolescence & Young Adulthood |
|
| Primary Prevention | |||
| Secondary Prevention |
Dads for Life Program | ||
| Tertiary Prevention | Child-Parent Psychotherapy |
Promising Prevention Programs
| Adolescence & Young Adulthood |
Adulthood | |
| Primary Prevention | ||
| Secondary Prevention | Changing Places Program | |
| Tertiary Prevention |
Moderate Intensity Family Violence |
Developing Protective Resources & Resilience
In addition to reducing negative behaviours and minimizing the adverse consequences of violence, another important aspect of prevention involves developing protective resources and competencies which may be especially valuable to high-risk young children and their families.
Examples of protective factors include: selfregulation, self-determination/self-efficacy, emotional literacy, social problem solving, help-seeking behaviours, intellectual capacity, school bonding and extracurricular involvement, community involvement, and positive interpersonal/family relationships.
One example of a program that supports the development of resilience is the Strengthening Families Program.
Prevention Programs with Applications across Life Stages
| Evidence-Based Programs | Promising Programs | |
| Primary Prevention | ||
| Secondary Prevention | ||
| Tertiary Prevention |
Considerations for Future Research
Data Collection
- Enhance data collection on child maltreatment and IPV (e.g. prospective longitudinal studies following children from birth with the capacity to control for potential confounding factors) and dissemination of findings to relevant stakeholders.
- Increase longitudinal research on risk and resiliency among maltreated children, including those exposed to IPV.
- Collect data on partner violence outcomes for maltreated boys who have and have not received treatment.
Program Development & Evaluation
- Enhance empirical evaluation of the long-term effectiveness of prevention programs (e.g. Neighbours, Friends and Families; White Ribbon Campaign).
- Develop and evaluate programs designed to restore parent-child relationships after violence has occurred.
- Develop and evaluate culturally relevant and gender-responsive programs for boys and men.
- Develop and evaluate programs designed to prevent IPV perpetration among boys who experienced maltreatment in childhood.
- Develop and evaluate differential responses to IPV perpetrators (e.g. based on type of violence, background, etc).
- Determine sufficient treatment levels in tertiary programs for IPV perpetrators.
Considerations for Practice
Training:
- Integrate IPV curricula into schools of public health, nursing, and medicine as well as related fields (e.g. social work, justice sector).
- Provide ongoing opportunities for cross-training on IPV and the victimization experiences of boys/men from a health perspective.
Collaboration:
- Develop partnerships between public health and local IPV programs.
- Promote coordinated community responses to IPV through development of multidisciplinary task forces involving researchers, service providers, and policy makers.
- Engage in multi-level prevention efforts involving communities, families & individuals.
Service Provisions:
- Address IPV and child maltreatment (abuse, neglect, IPV exposure) in tandem, including identifying shared risk factors, particularly in adolescent and young adult populations.
- Include the prevention of future IPV perpetration as an explicit goal in child maltreatment prevention programs.
- Increase services to ensure well-being after violence has ended.
- Multi-dimensional screening and follow-up for boys who have experienced abuse/neglect or who have been exposed to IPV, especially when other risk factors are present (e.g. little social support).
System Approaches:
- Conduct community needs assessments.
- Develop, implement, and monitor protocols for IPV in public health agencies.
- Increase funding for public health approaches to violence prevention.
- Invest in early prevention programs (e.g. dating violence prevention in adolescence with particular emphasis on boys with histories of victimization).
Written by the Learning Network Team:
Linda Baker, Learning Director
Nicole Etherington, Research Associate
Elsa Barreto, Graphic Design
Please evaluate us!
Let us know what you think. Your input is important to us. Please complete this brief survey on your thoughts of this newsletter: https://uwo.eu.qualtrics.com/jfe/form/SV_3qp8ixEOK0y2fOd
- WHO, 2007.
- Haegrich & Hall, 2011.
- Smith et al., 2011; Renner & Whitney, 2012; Millett et al., 2013.
- Public Health Agency of Canada, 2010.
- Hamby et al., 2010.
- Maguire et al., 2015.
- Bandura, 1977; Eriksson & Mazerolle, 2015.
- Bowlby, 1969; Levendosky et al., 2012.
- It is important to remember that not all perpetrators of IPV have experienced abuse, neglect, or IPV exposure and that there can be many different pathways leading to IPV perpetration. Additionally, not all studies find strong support for this link.
- For the purposes of this newsletter, we defined “evidence-based” as studies which used randomized control trials; however, we recognize that there are other forms of evidence that can be used to inform policy and practice.



